
Hip Replacement vs Knee Replacement: Which Is More Painful?
When a surgeon mentions joint replacement, most patients immediately want to know: hip replacement vs knee replacement, which is more painful? It's not a shallow question. It comes from a very real place of anxiety about what recovery will actually feel like, and it deserves a straight answer rather than vague reassurance.
The research is fairly clear. Studies consistently show that one procedure produces more post-operative pain than the other. Understanding why can help you prepare better, ask smarter questions, and set realistic expectations before reaching the operating table.
If you're weighing your options and want to find a verified orthopaedic specialist in Western Australia, Best Orthopaedic Surgeons (BOS) is designed to help patients search for specialists by location and subspecialty.
This article covers what the evidence says about pain levels for each procedure, the anatomical reasons behind the difference, what pain resolution looks like over weeks and months, how surgeons manage it, and the questions worth raising before surgery.
Hip Replacement vs Knee Replacement: Which Is More Painful?
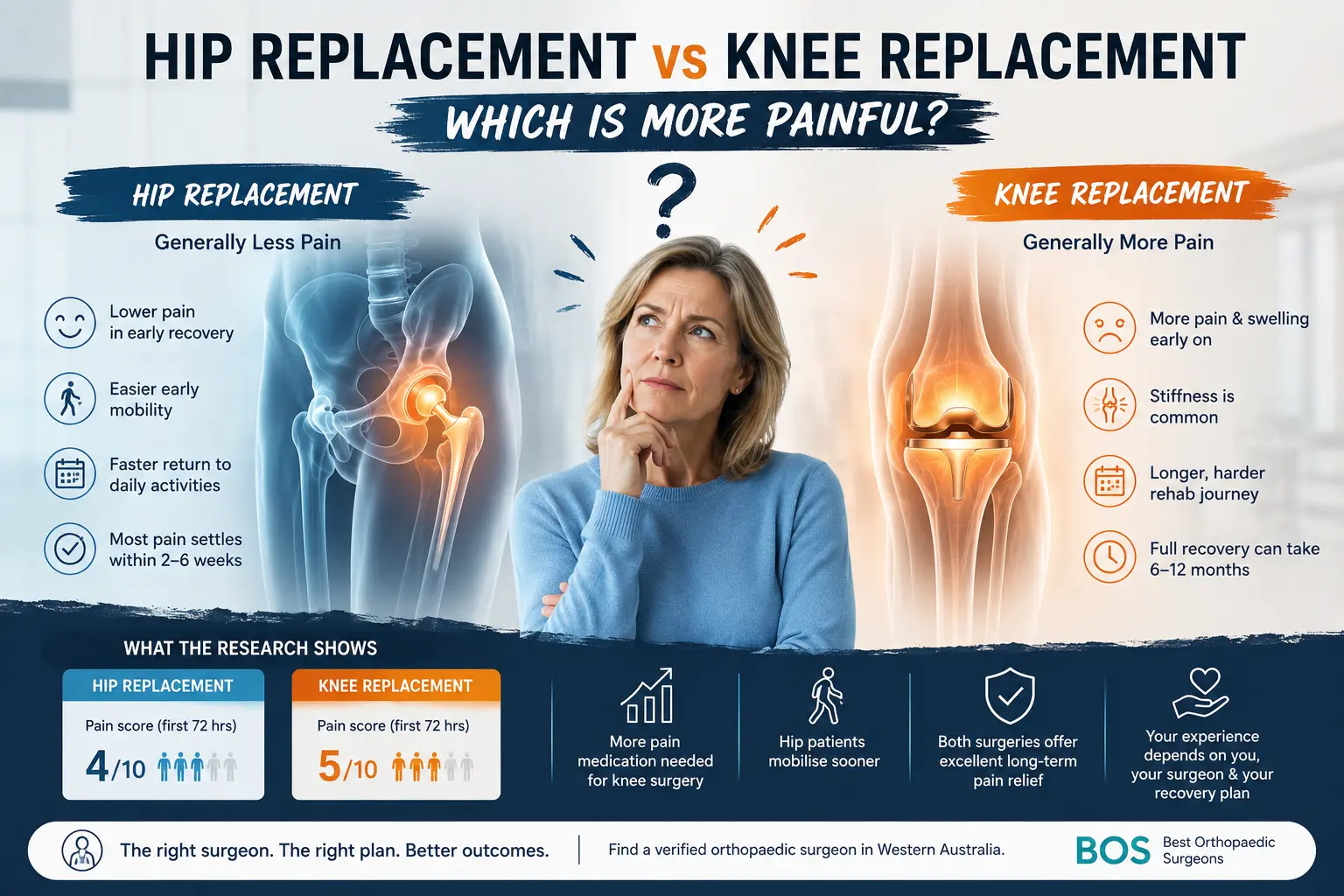
Knee replacement is generally more painful than hip replacement during the early post-operative period and throughout the initial rehabilitation phase.
Total knee arthroplasty usually produces higher early pain scores, greater swelling, more stiffness, and a longer rehabilitation process than total hip arthroplasty. Individual experiences still vary considerably, and modern pain-management techniques can make both procedures more manageable.
What the Evidence Shows
Multiple reviews and clinical studies have found that total knee arthroplasty, commonly abbreviated as TKA, produces higher post-operative pain scores than total hip arthroplasty, or THA, during the early recovery period.
In one widely cited study, the mean acute pain score during the first 72 hours was approximately 5 out of 10 for knee replacement patients and 4 out of 10 for hip replacement patients.
Moderate to severe pain affected approximately 51% of knee replacement patients compared with about 29% of hip replacement patients within the same study group.
Under modern multimodal pain management, hip replacement patients may report pain levels of approximately 2-4 out of 10 at rest during the first 24 hours, increasing to around 4-6 with movement.
Knee replacement patients may report approximately 4-6 out of 10 at rest and 6-8 out of 10 during movement in the same period.
These numbers represent population averages. Your experience may differ depending on surgical technique, anaesthesia, medication, pre-existing pain, general health, and individual pain sensitivity.
Opioid Use and Hospital Recovery Reflect the Same Pattern
The difference is not limited to pain scores. Knee replacement patients also tend to require more pain medication after surgery.
Some research has reported average opioid consumption of approximately 416 mg in oral morphine equivalents after knee replacement compared with around 285 mg after hip replacement.
Hip replacement patients also tend to mobilise earlier and with less difficulty. This can support faster discharge and earlier participation in rehabilitation.
The combination of lower early pain scores, reduced opioid requirements, and quicker mobility often makes the initial hip replacement recovery experience feel smoother.
Why the Knee Tends to Hurt More After Surgery
The Anatomy Behind the Difference
The knee is a complex and relatively superficial joint. Performing a total knee replacement requires reshaping several bone surfaces and working around ligaments, muscles, tendons, and the joint capsule.
This produces significant inflammation in the tissues surrounding the joint. The nerve supply around the knee is also dense and distributed across a wide area, which can make complete pain control difficult.
The hip sits deeper within the body and is surrounded by large muscle groups. Although these tissues are still affected during surgery, modern hip replacement approaches are designed to minimise unnecessary muscle and soft-tissue damage.
The hip's deeper position and the development of less disruptive surgical techniques can contribute to lower levels of early surface-level pain and inflammation.
Rehabilitation Demands Drive the Discomfort
A major reason knee replacement patients experience sustained discomfort is the rehabilitation itself.
Regaining knee flexion requires repeatedly bending a swollen and healing joint. These exercises must begin early because insufficient movement can lead to long-term stiffness and reduced range of motion.
That process can be genuinely uncomfortable, particularly during the first several weeks.
Hip replacement rehabilitation also involves range-of-motion exercises and gradual strengthening, but it generally does not require the same repeated bending of a swollen joint through a painful arc.
Hip replacement patients may describe rehabilitation as tiring but manageable, while knee replacement patients often describe physiotherapy as one of the hardest parts of the recovery.
Pain Timeline: Hip Replacement vs Knee Replacement
The First Few Days to the First Few Weeks
For hip replacement patients, pain is commonly moderate during the first 24-48 hours and improves steadily from that point.
Many patients begin walking with support within a day or two of surgery. With an appropriate pain-management plan, the sharpest post-surgical pain often begins settling within approximately two weeks.
Knee replacement usually follows a more demanding pain trajectory. The first two to three days are commonly the most intense.
Soreness, stiffness, swelling, and warmth around the knee may continue for three to six weeks. The joint can remain warm or swollen even after the surgical wound has healed.
Acute pain after both operations commonly improves within two to four weeks, but the knee often takes longer to feel settled.
The Three-Month and Twelve-Month Picture
Hip replacement patients often report feeling significantly better than they did before surgery by the three-month mark.
Most achieve near-complete pain relief between six and twelve months. Long-term satisfaction is high, with approximately 90-95% of patients reporting near-total pain relief in some studies.
Knee replacement follows a slower trajectory. Most daily activities may be manageable by three months, but full strength, flexibility, and endurance commonly take six to twelve months to recover. For a detailed week-by-week breakdown, see our guide on how long hip vs knee replacement recovery takes.
For some patients, meaningful improvements continue for as long as eighteen months.
Persistent pain rates at twelve to twenty-four months have been reported at approximately 12-15% after knee replacement. Some large patient groups report bothersome chronic pain in approximately 20-25% of patients.
These figures still mean that most patients achieve a good outcome. Understanding the longer timeline beforehand can prevent discouragement caused by expecting recovery to happen faster than it realistically will.
How Surgeons Manage Pain Differently for Hip and Knee Replacement
Modern joint replacement pain management generally uses several techniques together rather than relying on a single medication.
This approach is commonly called multimodal analgesia and may include regional nerve blocks, spinal anaesthesia, local injections around the joint, anti-inflammatory medication, paracetamol, and carefully controlled opioid medication when required.
Regional Nerve Blocks for Hip Replacement
Common regional techniques for total hip arthroplasty include the PENG block, or pericapsular nerve group block, and fascia iliaca blocks.
These approaches are intended to reduce pain while preserving enough muscle function for early mobilisation.
The PENG block targets nerves supplying the hip capsule and may help control pain without producing significant quadriceps weakness.
Regional blocks may be combined with spinal anaesthesia and local infiltration medication administered by the surgeon. This can reduce opioid requirements and help patients begin walking relatively soon after surgery.
Regional Nerve Blocks for Knee Replacement
For total knee arthroplasty, the adductor canal block has become a commonly used regional technique.
It is designed to reduce pain while preserving quadriceps strength more effectively than a traditional femoral nerve block.
Femoral nerve blocks can provide strong pain relief but may cause enough weakness to delay safe walking and increase the risk of falls.
The adductor canal block aims to balance effective pain control with early mobility.
Surgeons may also use periarticular injections and, in selected situations, continuous nerve catheters to extend pain relief.
When combined with anti-inflammatory medication and targeted oral analgesics, these protocols have made knee replacement recovery considerably more manageable than it was in the past.
Long-Term Pain Outcomes and Factors That Shape Recovery
Persistent Pain Rates by Procedure
At three months after surgery, approximately 22% of knee replacement patients may still report some level of pain.
That figure may fall to approximately 12-15% at twelve to twenty-four months.
Hip replacement outcomes are generally more favourable, with approximately 90-95% of patients achieving near-total pain relief.
The proportion of patients experiencing significant pain beyond twelve months is smaller after hip replacement than after knee replacement.
These numbers represent averages across large patient groups. They do not determine your personal outcome. Surgical technique, surgeon experience, medical history, and participation in rehabilitation all influence recovery.
Patient Factors That Can Affect Pain
Pre-operative opioid use is one of the strongest predictors of poorer pain outcomes after either procedure.
Patients who are already using opioids long-term before surgery may experience more difficult post-operative pain control, slower resolution of pain, and poorer functional outcomes.
If this applies to you, discuss it with your surgeon and GP well before the operation. Medication reduction should only be attempted with appropriate medical supervision.
A higher body mass index is also associated with increased post-operative pain, higher medication requirements, and slower recovery, particularly at very high body weights.
Building baseline fitness through safe, low-impact activity and improving overall health before surgery may support a smoother recovery.
Questions to Ask Before Your Surgery
Walking into a pre-surgical consultation with specific questions can improve the quality of the discussion.
Consider asking your orthopaedic surgeon:
- What nerve block protocol do you use for this procedure, and why?
- What pain level should I realistically expect during the first 48 hours?
- What does your multimodal pain-management plan include?
- How often do your patients require opioids after leaving hospital?
- How do you help patients safely reduce pain medication?
- What physiotherapy support will be available during the first two weeks?
- How might my current health, body weight, fitness, and medication use affect recovery?
These questions provide practical, personalised information and show your surgeon that you expect clear communication about pain and recovery.
Finding a Verified Specialist Who Will Give You Straight Answers
Getting honest and personalised answers depends on finding the right surgeon.
Not every orthopaedic specialist has the same experience with hip and knee replacement, and not every clinic follows the same pain-management protocol.
For patients in Western Australia, Best Orthopaedic Surgeons (BOS) makes the search more straightforward.
Through BOS, patients can:
- Filter verified surgeons by hip or knee subspecialty
- Review detailed surgeon profiles
- Read patient reviews
- Search by location, including Perth
- Ask questions through the platform
- Find educational information about joint replacement
This focus can help patients identify a surgeon with relevant experience instead of navigating a broad healthcare directory and hoping the selected specialist regularly performs the procedure being considered.
The Takeaway Worth Remembering
So, hip replacement vs knee replacement: which is more painful?
The evidence consistently indicates that knee replacement produces higher early pain scores, greater opioid requirements, more swelling and stiffness, and a longer recovery journey.
Modern multimodal pain management, including targeted nerve blocks and anti-inflammatory protocols, has made the experience significantly more manageable than it once was.
Most patients undergoing either procedure still achieve strong long-term outcomes.
Your personal health factors matter as much as the procedure itself. Improving baseline fitness, managing weight where appropriate, addressing long-term opioid use with your doctor, and understanding the realistic recovery timeline can improve your preparation.
The best preparation for either operation is a detailed conversation with a surgeon who understands your case.
If you're in Western Australia and looking for that specialist, start with Best Orthopaedic Surgeons (BOS). Search by subspecialty, review surgeon profiles, and read patient feedback, and prepare your questions before booking.
Frequently Asked Questions
Is Hip Replacement or Knee Replacement More Painful Overall?
Knee replacement is generally more painful than hip replacement during both the immediate post-operative period and early rehabilitation. Knee replacement patients tend to report higher pain scores, use more pain medication, and take longer to reach full recovery.
How Long Does Pain Last After Knee Replacement Compared with Hip Replacement?
After hip replacement, many patients find that acute pain begins settling within approximately two weeks, with continued improvement over six to twelve months.
After knee replacement, significant discomfort, swelling, and stiffness may continue for three to six weeks. Full strength and endurance recovery commonly takes twelve months and may continue for up to eighteen months.
What Is the Persistent Pain Rate After Each Procedure?
Approximately 5-10% of hip replacement patients may experience persistent pain at twelve months.
For knee replacement, the figure is commonly reported at approximately 12-15%, with some large patient groups reporting bothersome chronic pain in up to 20-25% of patients.
What Can I Do Before Surgery to Reduce Post-Operative Pain?
Helpful preparation may include improving baseline fitness through appropriate low-impact exercise, optimising general health and body weight where recommended, and discussing any long-term opioid use with your GP and surgeon.
Do not stop or change prescribed medication without guidance from a qualified healthcare professional.