
Your MRI is back. The ACL is torn. Surgery is recommended. And then your surgeon leans forward and asks a question you weren't expecting: "Have you thought about what type of graft you'd prefer?" Understanding ACL graft types before that conversation means you walk in informed rather than overwhelmed. If your first reaction is a blank stare, you're not alone, many patients have never heard terms like bone-patellar tendon-bone, hamstring autograft, or allograft, yet they're being asked to weigh in on one of the most consequential decisions of their recovery.
This guide breaks down the four main ACL reconstruction grafts in plain language: bone-patellar tendon-bone (BPTB), hamstring tendon, quadriceps tendon, and allograft (donor tissue). Each has a different complication profile, a different rehab emphasis, and a different evidence base depending on who you are and what you're returning to. Understanding the differences puts you in a far better position to have a productive conversation with your surgeon rather than just nodding along.
For patients in Western Australia, Best Orthopaedic Surgeons (BOS) connects you with orthopaedic surgeons who specialise in ACL reconstruction across Perth and regional WA. You can search by subspecialty, read patient reviews, and book a consultation with someone who can match the right graft to your specific situation. By the end of this guide, you'll understand exactly what sets each option apart.
What the four main ACL graft types actually are
Before comparing ACL grafts side by side, it helps to understand the core split. An autograft uses tissue harvested from your own body, while an allograft uses pre-processed donor tissue from a cadaver. Autograft is generally preferred in younger and active patients because the evidence consistently shows lower failure rates than allograft in that population. Allograft eliminates the need for a second harvest site, which sounds appealing, but it comes with meaningful trade-offs covered later in this guide.
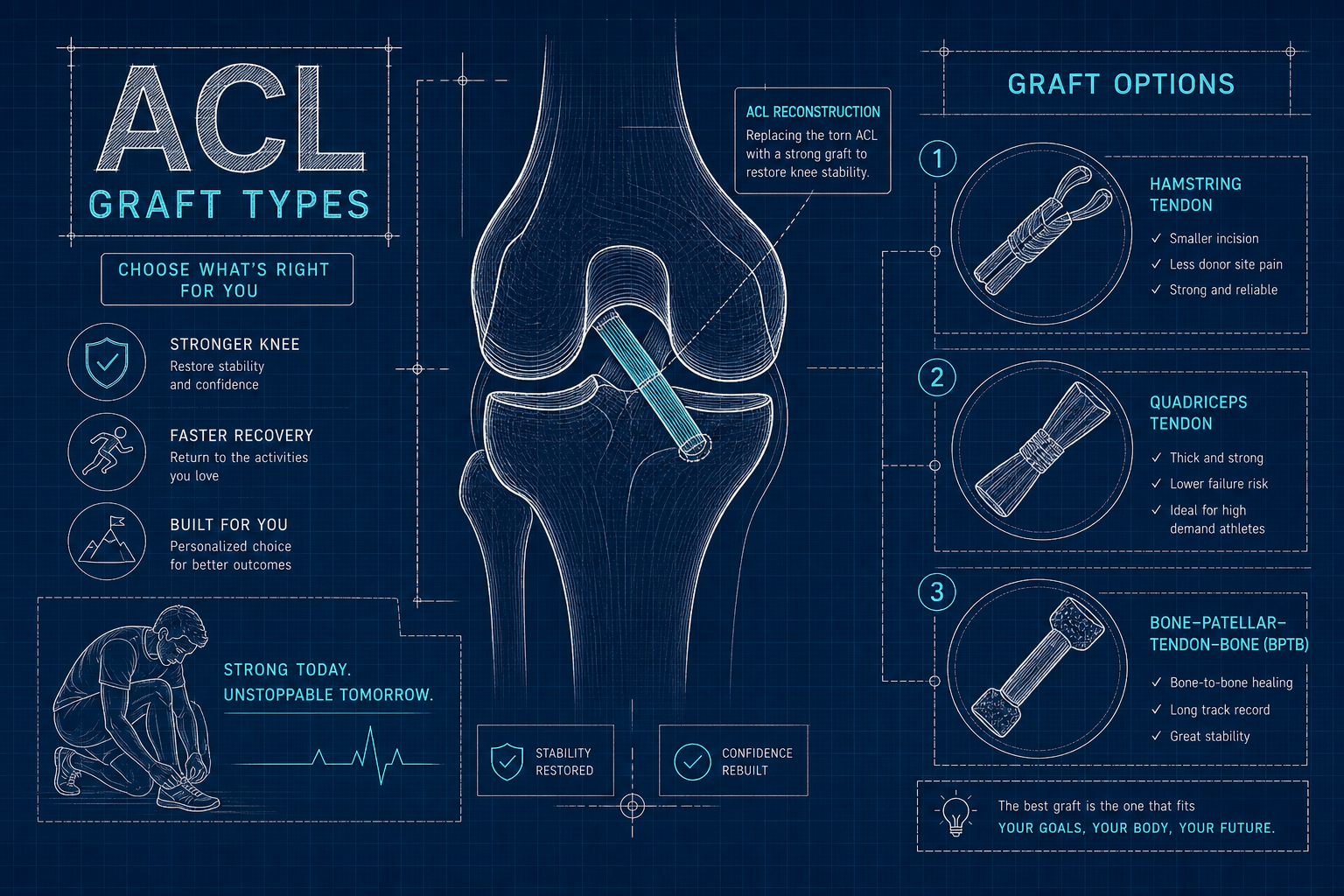
Within the autograft category, there are three main sources surgeons draw from. The BPTB graft takes the central third of the patellar tendon, with bone plugs at each end from the patella and tibial tubercle, fixed into drilled tunnels using interference screws. This bone-to-bone contact is one of its key mechanical advantages. The hamstring tendon graft typically uses the semitendinosus, sometimes combined with the gracilis, folded into a quadruple-strand structure and fixed with suspensory buttons. The quadriceps tendon graft is harvested from the thick tendon above the kneecap, available with or without a bone plug, and is increasingly chosen for its naturally large cross-sectional size. Each of these sits in a different part of the leg, which matters enormously when you start thinking about recovery.
ACL graft types compared: BPTB versus hamstring autograft
These two ACL grafts have been studied head-to-head in the literature for decades. BPTB remains the preferred choice for many high-demand athletes: bone-to-bone healing is faster and more predictable, objective knee stability tends to be slightly superior, and failure rates in young and active populations are generally lower than hamstring autograft. A 2022 meta-analysis reported approximate graft failure rates of 5.1% for BPTB versus 11.1% for hamstring in patients under 25, differences that matter significantly for anyone planning to return to pivoting sports.
The trade-off is significant, though. Anterior knee pain affects a notable proportion of patients post-harvest, and kneeling discomfort is reported in a substantial share of BPTB cases in short-term studies; long-term follow-up data shows lower rates, but kneeling-related discomfort can persist for some patients. For tradespeople, athletes who kneel frequently, or anyone with a physically demanding lifestyle, that's a real quality-of-life consideration that deserves a direct conversation with your surgeon before you decide.
Hamstring autograft appeals for different reasons: less anterior knee pain, a less invasive harvest, and solid overall functional outcomes. The critical nuance is graft diameter. Grafts smaller than 8 mm carry a measurably higher re-rupture risk, with one study reporting failure rates of approximately 9.5% for grafts at or below 7.5 mm compared to 2.1% for grafts in the 8 to 8.5 mm range. Patients with naturally smaller tendons may not be able to produce an adequate hamstring graft, which changes the equation entirely. Sensory numbness around the harvest site is also common, reported across a wide range in the literature (roughly 40, 88% in some studies, lower in others), though it is usually temporary rather than permanent.
Quadriceps tendon: the rising ACL graft option backed by strong evidence
Many patients haven't heard of the quadriceps tendon graft because it wasn't widely used until relatively recently. That's changing fast, and the evidence is driving it. The quadriceps tendon is one of the thickest tendons in the body, giving surgeons a naturally large graft that is straightforward to prepare. Recent systematic reviews report failure rates comparable to BPTB in young athletes, with a 2022 meta-analysis placing quad tendon failure at approximately 2.5% in patients under 25, the lowest of the three autograft options in that dataset. It's worth noting that the evidence base continues to develop, and readers should discuss the most current findings with their surgeon.
The kneeling pain profile is also more favourable. Kneeling pain is reported in roughly 19% of quad tendon patients compared to higher rates with BPTB, which makes it a more comfortable long-term option for active patients. For anyone whose sport or profession involves frequent kneeling, this distinction is clinically meaningful.
The main donor-site concern with quad tendon is quadriceps muscle atrophy, reported in approximately 38% of cases in some studies compared to around 25% with BPTB. The 38% figure reflects measurable atrophy, not permanent weakness, targeted physiotherapy resolves it in the majority of cases. What it does mean is that the early rehab phase needs to prioritise quadriceps activation from week one. Patients who understand this going in tend to engage with that phase more seriously, which translates to better outcomes.
Allograft: when donor tissue is a reasonable choice
Allograft is a legitimate option, but only in the right patient profile. The evidence on failure rates in younger and active patients is consistently unfavourable. Systematic reviews show allograft carries a higher re-rupture rate than autograft across the board, with the gap widest in patients under 25 and those returning to pivoting or cutting sports. Irradiated or heavily processed allografts perform worst of all. For competitive athletes, most clinical guidelines recommend autograft as the primary choice, and that recommendation is well-supported by the literature.
That said, allograft is not dismissed by experienced surgeons. It makes genuine sense in specific profiles: older patients with lower activity demands, revision ACL cases where autograft tissue has already been used or is compromised, and multiligament injury reconstructions where donor-tissue options are limited. No second harvest site means lower operative complexity and no harvest-related complications, a real advantage in cases where long-term athletic durability is not the primary concern.
How surgeons actually decide: age, anatomy, and revision status
The graft selection process is not a simple menu choice. Surgeons weigh a specific combination of patient-level factors before recommending an approach. Age is the starting point: younger patients skew strongly toward autograft because their failure risk is already elevated by activity level and biological demands. Activity type matters too. High-demand pivoting athletes benefit from grafts with the lowest documented failure rates, which currently means BPTB or quad tendon in the under-25 population.
Anatomy plays a direct role. If preoperative imaging or intraoperative assessment suggests the hamstring tendons are small, a surgeon may steer toward BPTB or quad tendon to avoid an undersized graft. Some subgroup analyses suggest BPTB may outperform hamstring in certain young female populations, though that evidence is preliminary and should be discussed individually. Sex-related anatomical differences in tendon size and joint geometry are real factors that an experienced ACL surgeon will factor into the recommendation.
Revision ACL reconstruction introduces a different set of considerations entirely. If the original surgery used a hamstring autograft, the surgeon will generally choose a different source the second time. That might mean ipsilateral quad tendon, contralateral harvesting, or allograft when other options are exhausted. Concomitant injuries such as meniscal tears or posterolateral corner damage also affect the overall reconstruction strategy and can indirectly influence graft selection based on what the knee will be asked to tolerate.
ACL graft types and recovery timelines: what to actually expect
Graft type changes the focus of rehabilitation more than it changes the overall calendar. Most patients, regardless of which graft is used, are looking at 9 to 12 months before returning to pivoting sport. Cohort data from competitive athletes suggests BPTB patients typically reach return-to-sport criteria at around 10 to 12 months, hamstring autograft patients at roughly 8 to 10 months, and quad tendon patients at approximately 9 to 11 months. These are averages with meaningful variation depending on concomitant injuries, post-operative swelling, and rehabilitation consistency.
The practical rehab differences break down like this:
- BPTB patients need extra focus on managing anterior knee pain and restoring full knee extension early, which can slow quadriceps loading in the initial weeks.
- Hamstring autograft patients require careful early loading of the harvest site and deliberate hamstring strengthening throughout the mid-phase.
- Quad tendon patients prioritise quadriceps activation from week one to counter the atrophy risk at the donor site.
- Allograft patients typically follow a more conservative protocol because biological graft incorporation takes longer without the cellular response that autograft tissue triggers.
For active patients asking "when can I play again?", the honest answer is that elite athletes average 9.5 to 10.7 months depending on sport, with concomitant meniscal injury and persistent post-op effusion being the most common factors that push the timeline out. Recreational patients follow a similar window if they pursue full sport return. Criteria-based clearance, covering strength symmetry testing, hop assessments, and movement quality, matters far more than hitting a specific date on the calendar. A green light at nine months means less than passing the right tests at ten.
Making the decision: what to take into your surgical consultation
The key takeaways from the evidence are clear. BPTB and quadriceps tendon autografts offer the lowest documented failure risk in young, active patients. Hamstring autograft is a strong choice when graft diameter is adequate and the patient's anatomy supports it. Allograft is best reserved for older, lower-demand patients or revision cases where autograft tissue is limited. No two ACL reconstructions are identical, and the right ACL graft for a 19-year-old AFL player is not the right ACL graft for a 52-year-old recreational cyclist.
Before your consultation, it's worth preparing specific questions: What graft do you recommend for my age and activity level, and why? What is my expected hamstring diameter, and does that influence your recommendation? Have you performed this procedure with each graft type, and what outcomes have you seen? What would change your recommendation if a different graft type is chosen?
Understanding ACL graft types is one of the most important steps you can take before surgery, and the decision deserves a surgeon who specialises in this area. For patients in Western Australia, Best Orthopaedic Surgeons (BOS) gives you a straightforward way to find orthopaedic surgeons across Perth and regional WA who focus on ACL reconstruction and sports-related knee injuries. Use the platform to compare surgeon profiles, read patient reviews, and book a consultation with a specialist who can match the right ACL graft type to your anatomy, your sport, and your recovery goals.